13Y OLD FEMALE WITH SICKLE CELL CRISIS
1st February 2022
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent.
Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs.
This Elog book also reflects my patient-centred online learning portfolio and your valuable inputs on the comment .
Patient and his/her attenders have been informed and their consent has been taken.
A 13 YEAR OLD GIRL WITH ABDOMINAL PAIN AND VOMITTINGS.
HOPI
She is second born child of parents married of 3rd degree consanguinity in 2009. All trimesters were uneventful. She was delivered through Caeserean section because of delayed labour pain with birth weight of 3kg.
Immusnized till date.
2012
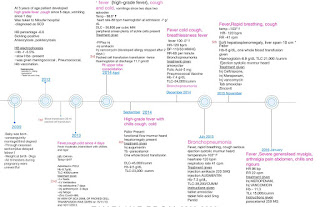
She was asymmtomatic upto age of 3 years, then she developed high grade fever with cough and vomittings. She was diagnosed with Sickle cell anaemia. Sickling test positive and Electrophoresis showed HbS. Blood transfusion were given 1packet.
2013
She developed high grade fever, dry cough and cold. She was diagnosed with Bronchopneumonia. X-ray lower lobe consolidation.
2015
She had recurrent episodes of fever, cough , cold i.e Recurrent Bronchopneumonia- 6 episodes in 3years. Urine culture showed Klebsiella growth.
Blood transfusion till date 4 times.
2016
She developed fever, pain abdomen , myalgia and arthralgia. She improved on medications and thus was discharged.
2019
She came with stomach pain and vomittings. She was diagnosed to have Acute pancreatitis.
2022
She developed stomach pain last night which was sudden in onset, gradually progressive, pricking type in epigastrium, left hypochondrium, aggravates on walking.
She had 2episodes of vomitting- watery, non bilious, projectile. Dark coloured stools and dark urine.
No history of constipation, difficulty in swallowing, burning sensation.
She is immunized till date.
Since 2years she did not have any blood transfusion. Before that whenever she had fever, she was transfused blood after investigations.
All developmental milestones achieved till date.



PAST HISTORY
Known case of Sickle cell Anemia.
History of Bronchopneumonia.
History of 8 PICU admissions.
Previous blood transfusions.
No history of Asthama, Thyroid Tuberculosis, Hypertension, Diabetes, Epilepsy.
TREATMENT HISTORY
Hydroxyurea 1000mg/day
Tab Pentid 600mg/day
Tab Folnite 5mg/day
Tab Sodamint
Tab Calcium 500mgBD
Tab Zevit OD
Tab Ecospirin 75mg at night
FAMILY HISTORY
Not significant
PERSONAL HISTORY:
Appetite - Normal
Diet - Non vegetarian
Bladder and bowel movements - Regular
Sleep - Adequate
No known allergies
No addictions.
GENERAL EXAMINATION:
Patient was conscious, coherent and cooperative. Well oriented to time, place and person.
Pallor present
Icterus present
Cyanosis, clubbing, lymphadenopathy, Pedal edema absent
Height - 138cm
Weight - 35kg
Vitals
Temp: Febrile
PR- 105Min
RR- 24/Min
BP- 110/70 mmHg
Spo2 -99%at RA
SYSTEMIC EXAMINATION
P/A - Shape of abdomen- Normal. Umbilicus everted. No scars. On palpation - Soft, tender, liver palpable. Bowel sounds heard.
CVS- S1 S2 heard, no murmurs
RS- NVBS.
CNS- NFND
Tone, power and reflexes are normal.










INVESTIGATIONS
Hb - 7.9gm/dl
TLC- 16,400
ESR - 20 min
Blood group - O positive
Total Bilirubin - 20.15
Direct Bilirubin - 14.13
SGOT - 170
SGPT - 180
ALP - 560
CRP negative
Serology - Negative
Amylase - 994
LDH - 543
Blood urea - 13
Creatinine - 0.4
Electrolytes : Na 140, K 4.2 , Cl 101

Plueral tap

PROBABLE DIAGNOSIS
VASO-OCCLUSIVE CRISIS in SICKLE CELL ANAEMIA
ACUTE PANCREATITIS
ARDS secondary to? Pnuemonia or? Pulmonary Infarction
PLUERAL EFFUSION secondary to? consolidation
TREATMENT
IVF NS and DNS
Inj PAN 40mg/day
Inj OPTINUERON
Inj DICLO
DISCUSSION





https://pubmed.ncbi.nlm.nih.gov/12827657/#:~:text=Acute%20pancreatitis%20is%20rarely%20included,of%20microvessel%20occlusion%20causing%20ischemia.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5139833/


Comments
Post a Comment